This is going to be a comprehensive, detailed document covering everything about MY specific mutations and a thorough general genetics education section THIS WILL BE IN PART TWO. – Please note anything highlighted yellow either means its a start of a new topic , its important or it specifically indicates my specific case.
PART ONE: MY SPECIFIC MUTATIONS — COMPLETE ANALYSIS
THE RYR1 GENE — FOUNDATIONAL UNDERSTANDING
Before analyzing MY specific mutations, understanding the gene itself is essential, i know i posted about the basic information on the gene in the last blog but i want to go over the understanding here as well before i get into my Gene mutations so its more clear.
Gene Location and Size
Chromosome: 19 (specifically 19q13.2 — the long arm of chromosome 19, region 13, band 2)
Total size: Approximately 150,000 base pairs of DNA
Number of exons: 106 (coding segments)
Total protein length: 5,037 amino acids
Classification: One of the largest known human genes
- The RYR1 Protein Structure — Critical for Understanding Mutation Effects
- The RYR1 protein functions as a homotetramer — meaning four identical RYR1 protein subunits must assemble together to form one functional calcium channel complex. This assembly is critical because:
- Each subunit is enormous (5,037 amino acids, ~560 kilodaltons)
- Four subunits together create a channel weighing approximately 2.2 megadaltons — one of the largest known protein complexes in biology
- If even ONE subunit is severely dysfunctional, it can disrupt the entire tetramer
- The RYR1 protein functions as a homotetramer — meaning four identical RYR1 protein subunits must assemble together to form one functional calcium channel complex. This assembly is critical because:
- The protein has distinct structural and functional zones:
- N-terminal cytoplasmic domain (approximately aa 1–3,600):
- Forms the massive “foot” structure visible under electron microscopy
- Contains regulatory binding sites for dozens of other proteins (calmodulin, FKBP12, PKA, calsequestrin, triadin, junction)
- Contains the “hot spot” regions where most pathogenic mutations cluster
- Houses the allosteric regulation machinery — sites where signals from outside the cell (metabolic state, redox status, pH, temperature) modulate channel activity
- Central linker/regulatory domain (approximately aa 3,600–4,200):
- Connects the cytoplasmic regulatory domain to the transmembrane pore
- Contains critical inter-domain contacts that transmit conformational changes from regulatory sites to the pore
- MY maternal frameshift mutation falls at the BEGINNING of this region (aa 4,189) — disrupting the critical connection between the regulatory machinery and the channel pore
- Transmembrane/pore domain (approximately aa 4,200–5,037):
- Embeds in the sarcoplasmic reticulum membrane
- Forms the actual calcium-conducting pore
- Contains the selectivity filter — the molecular “gate” that allows Ca²⁺ through while blocking other ions
- Contains the luminal (SR interior) calcium sensing region
The Three Established RYR1 Mutation Hotspot Regions
Scientists have identified three regions of the RYR1 protein where pathogenic mutations cluster disproportionately:
- Hotspot 1: Approximately amino acids 35–614 (N-terminal)
- Hotspot 2: Approximately amino acids 2,163–2,458 (central)
- Hotspot 3: Approximately amino acids 4,136–4,973 (C-terminal) — MY MATERNAL MUTATION FALLS HERE
The fact that pathogenic mutations cluster in these regions — rather than being evenly distributed across the protein — tells scientists these regions are functionally critical and that mutations here disproportionately disrupt normal channel function.
MY MUTATION #1 (MATERNAL) — THE PATHOGENIC VARIANT
Full Designation
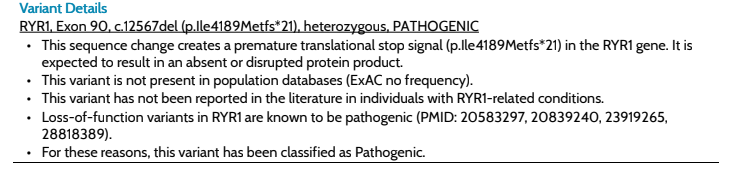
RYR1, Exon 90, c.12567del (p.Ile4189Metfs*21), heterozygous, PATHOGENIC
Breaking Down Every Part of This Name
- “RYR1” — The gene affected.
“Exon 90” — The location within the gene.- The RYR1 gene has 106 exons total
- Exon 90 is in the later portion of the gene — near but not at the very end
- At the protein level, exon 90 encodes amino acids in the critical C-terminal hotspot region (Hotspot 3)
- Exons in the C-terminal region of RYR1 encode the linker domain connecting regulatory machinery to the transmembrane pore — a structurally and functionally critical transition zone
- “c.12567del” — The DNA-level change.
- “c.” = coding sequence (the DNA that actually codes for protein, as opposed to regulatory/intronic regions)
- “12567” = the position number within the coding sequence where the change occurs (the 12,567th nucleotide of the coding sequence)
- “del” = deletion — one single nucleotide (one DNA “letter”) has been deleted at this position
- This is a single nucleotide deletion — the smallest possible type of deletion mutation
- “p.Ile4189Metfs*21” — The protein-level consequence.
- “p.” = protein (this part of the name describes what happens to the protein)
- “Ile” = Isoleucine — the amino acid that SHOULD be at position 4,189 in the normal protein
- “4189” = amino acid position 4,189 out of 5,037 total — approximately 83% of the way through the protein
- “Met” = Methionine — the first amino acid that is INCORRECTLY incorporated after the frameshift begins (because the reading frame has shifted, the codon at position 4,189 now reads as methionine instead of isoleucine)
- “fs” = frameshift — the critical descriptor; the deletion has shifted the reading frame
- “*21” = a premature stop codon appears 21 amino acids AFTER the frameshift begins — the protein is cut off at position 4,189+21 = approximately amino acid 4,210 instead of the normal 5,037
The Frameshift Mechanism — Explained In Complete Detail
To understand why a single deleted nucleotide causes such catastrophic consequences, MY and OUR need to understand how DNA is translated into protein.
The Genetic Code — Triplet Codons:
DNA is read in groups of three nucleotides called codons. Each codon specifies exactly one amino acid. The sequence of codons in a gene determines the sequence of amino acids in the protein.
Normal DNA: …AAT CGT TAC GGA TTC…
Codons: AAT | CGT | TAC | GGA | TTC
Amino acids: Asn | Arg | Tyr | Gly | Phe
What a single nucleotide deletion does:
When ONE nucleotide is deleted, every codon from that point forward is shifted by one position. This is the frameshift effect:
Normal: …AAT CGT TAC GGA TTC…
…Asn-Arg-Tyr-Gly-Phe…
After deleting one nucleotide (in this illustration, the “A” at position 1 of the second codon):
Mutated: …AAT GTT ACG GAT TC…
…Asn-Val-Thr-Asp-STOP?…
Every single codon from the deletion point forward reads completely differently — it’s like removing one space from a sentence and having every word after it scramble:
Normal: “THE CAT SAT ON THE MAT”
- Delete one letter: “THE ATS ATO NT HEM AT” — complete nonsense from the deletion point forward
The specific effect of c.12567del in RYR1:
- The single nucleotide deletion occurs at coding position 12,567
- From that point forward, every codon reads differently
- This means the amino acid sequence of the protein is COMPLETELY WRONG from position 4,189 onward
- After scrambling through 21 incorrect amino acids, the new reading frame generates a premature stop codon (UAA, UAG, or UGA in RNA)
- The ribosome (the cellular machine that builds proteins) stops when it hits this stop codon
- The resulting truncated protein would be approximately 4,210 amino acids long instead of the normal 5,037 — missing the entire C-terminal transmembrane and pore domain
BUT — the protein is almost certainly never even made:
The cell has a quality control system called Nonsense-Mediated Decay (NMD). NMD recognizes messenger RNA molecules that contain premature stop codons (specifically those that occur more than ~50-55 nucleotides before the last exon-exon junction) and degrades them before they can be translated into protein.
MY mutation’s premature stop codon in Exon 90 (of 106 total exons) almost certainly triggers NMD — meaning the cell destroys the mutant mRNA transcript before a truncated protein can even be produced. The end result is that this allele contributes essentially ZERO RYR1 protein to the cellular pool.
- This is the most severe possible mutation class: a null allele — producing nothing.
Why This Specific Location Matters
Position 4,189 sits at the beginning of the critical junction between:
The cytoplasmic regulatory domain (where the “decision” to open is made) - The transmembrane pore domain (where calcium actually flows through)
Even if NMD did NOT occur and a truncated protein WERE made, it would:
- Lack the entire transmembrane anchoring domain (cannot even insert into the SR membrane properly)
- Lack the pore-forming region (cannot conduct calcium)
- Lack the C-terminal regulatory regions that control channel gating
- Potentially act as a dominant negative if it could still dimerize with normal subunits — poisoning the tetramer assembly
In every scenario, this mutation produces no functional contribution to RYR1 channel activity from the maternal allele.
Population Frequency — The Significance of Zero
The fact that c.12567del is absent from all population databases — specifically from:
- ExAC (Exome Aggregation Consortium) — 60,706 individuals
- gnomAD (Genome Aggregation Database) — 141,456 exomes + 15,708 genomes (v2.1.1) and expanding versions
- dbSNP — does not have a registered rsID for this variant
- 1000 Genomes Project
- ESP (Exome Sequencing Project)
- Invitae’s own internal database of all tested individuals
and has never been published in the peer-reviewed literature in association with any other patient — tells us several important things:
- This mutation is so rare it has never been independently rediscovered in any sequenced human population worldwide
- Natural selection acts against it (individuals with this mutation have reduced reproductive fitness due to disease)
- It is almost certainly a de novo or very recently arisen mutation within the family lineage — not an ancient inherited variant that spread through a population
- It cannot be classified using the typical evidence framework (population frequency comparisons) because there is nothing to compare it to — its pathogenicity is determined by its MECHANISM (frameshift → premature
stop → NMD → null allele) rather than by frequency data
The clinical implication of zero population frequency: This variant exists in essentially no other human being on Earth currently known to science. MY maternal RYR1 allele is, to the best of current scientific knowledge, unique to MY and MY family line
Proof: this is my genetic report and what it states
ACMG Classification Criteria — Why “PATHOGENIC” Despite Novelty
The American College of Medical Genetics and Genomics (ACMG) has established a five-tier classification system for genetic variants:
- Pathogenic
- Likely Pathogenic
- Variant of Uncertain Significance (VUS)
- Likely Benign
- Benign
MY maternal variant received the highest-confidence classification: PATHOGENIC. Despite never having been seen before, it received this classification because the ACMG criteria include strong evidence categories that apply to MY variant even without prior reports:
PVS1 (Very Strong evidence — Pathogenic):
- Null variant (frameshift, nonsense, splice site, large deletion) in a gene where loss-of-function is a known disease mechanism. ✅
RYR1 is a well-established disease gene
- Loss-of-function variants in RYR1 are known pathogenic (PMIDs cited in the lab report: 20583297, 20839240, 23919265, 28818389)
- Your frameshift with premature stop → NMD → null allele is the prototypical PVS1 scenario
PM2 (Moderate evidence — Pathogenic):
- Absent from population databases in a recessive disease context. ✅
Zero frequency in ExAC/gnomAD
PP4 (Supporting evidence — Pathogenic):
Patient phenotype consistent with the gene-disease relationship. ✅
MY clinical presentation is consistent with RYR1-related myopathy
The combination of PVS1 alone is often sufficient for Pathogenic classification — the other criteria further support it. This is why a never-before-seen variant can be definitively called Pathogenic: the mechanism (not the frequency) determines pathogenicity for null alleles.
MY MUTATIONS #2, #3, AND #4 (PATERNAL) — THE VUS TRIO
These three variants are all on the SAME chromosome (in cis) — meaning they were inherited together as a single haplotype from MY father. This is critically important for interpretation
Mutation #2 (Paternal)
Full Designation:
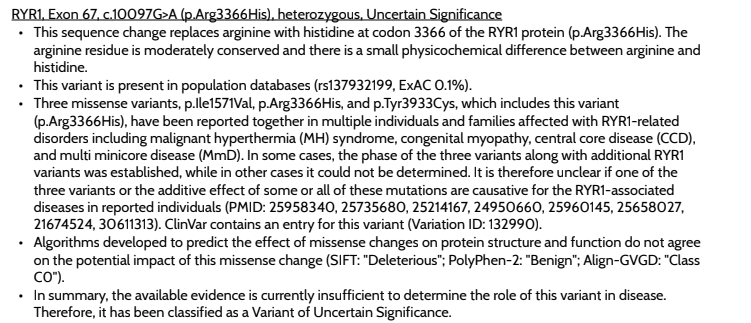
- RYR1, Exon 67, c.10097G>A (p.Arg3366His), heterozygous, Variant of Uncertain Significance
Breaking Down the Name
“Exon 67” — Approximately two-thirds of the way through the gene
- Located in the large cytoplasmic regulatory domain of the protein
- Not within the canonical hotspot regions (though close to the boundaries of Hotspot 2)
- This region contains important inter-domain communication pathways
“c.10097G>A” — DNA-level change
- Position 10,097 in the coding sequence
- “G>A” = a Guanine nucleotide has been replaced by an Adenine nucleotide
- This is a single nucleotide variant (SNV) — a substitution, NOT a deletion (completely different from your maternal mutation)
- One letter changed to another letter — the reading frame is NOT disrupted
“p.Arg3366His” — Protein-level consequence
- “Arg” = Arginine — the normal amino acid at position 3,366
- “3366” = amino acid position 3,366 out of 5,037
- “His” = Histidine — the amino acid that is INCORRECTLY present due to this mutation
- This is a missense mutation — a single amino acid substitution
The Arginine-to-Histidine Change — Why It Matters
Arginine (Arg, R):
- Positively charged at physiological pH
- One of the most basic (high pH) amino acids
- Frequently involved in electrostatic interactions with negatively charged residues, DNA, and phospholipids
- Often found at sites critical for protein-protein interactions and allosteric regulation
- The guanidinium group of arginine can form multiple hydrogen bonds simultaneously — making it a very “sticky” amino acid at interaction interfaces
Histidine (His, H):
- Partially positively charged at physiological pH (pKa ~6.0, so it’s transitioning between charged and uncharged near neutral pH)
- Much weaker positive charge than arginine
- Histidine is unique in being able to switch between protonated (charged) and neutral states near physiological pH — making it a frequent participant in enzyme active sites
- Cannot form as many or as strong hydrogen bonds as arginine
- Physically smaller than arginine
The physicochemical impact:
- Replacing a strong, consistently positively charged arginine with a weaker, partially-charged histidine at position 3,366 is a moderate physicochemical change — not as drastic as replacing a charged amino acid with a neutral or hydrophobic one, but not trivially benign either
- The Invitae report specifically notes “there is a small physicochemical difference between arginine and histidine” — a slight understatement of the actual charge and size differences
- At a site in the inter-domain communication region of RYR1, this change could alter local electrostatic interactions, protein-protein binding surfaces, or allosteric signal transmission
Population Frequency
- rsID: rs137932199
- ExAC frequency: approximately 0.1% (1 in 1,000 people in the database)
- Context: 0.1% is rare but NOT ultra-rare — this variant exists in the general population at low frequency
- Important interpretation: The presence of this variant at 0.1% frequency means it CAN exist in healthy individuals — arguing AGAINST it being fully penetrant dominant pathogenic on its own. However, in the context of recessive disease (combined with other variants on the same allele and the pathogenic null allele on the other chromosome), its individually modest frequency is less reassuring.
Computational Predictions (Contradictory — Hence VUS)
- SIFT: “Deleterious” — predicts this substitution disrupts protein function
- PolyPhen-2: “Benign” — predicts this substitution is tolerated
- Align-GVGD: “Class CO” — predicts no significant impact
- Interpretation: When computational tools disagree, no single prediction should be trusted — this disagreement itself supports VUS classification
ClinVar Entry
- ClinVar Variation ID: 132990
- Multiple submissions from different laboratories and families, with various interpretations — the fact that ClinVar contains an entry means this variant has been encountered before in clinical genetic testing, and the accumulating evidence is what keeps it in the VUS (rather than Benign) category
PROOF HERE: and what the genetic report states
Mutation #3 (Paternal)
Full Designation:
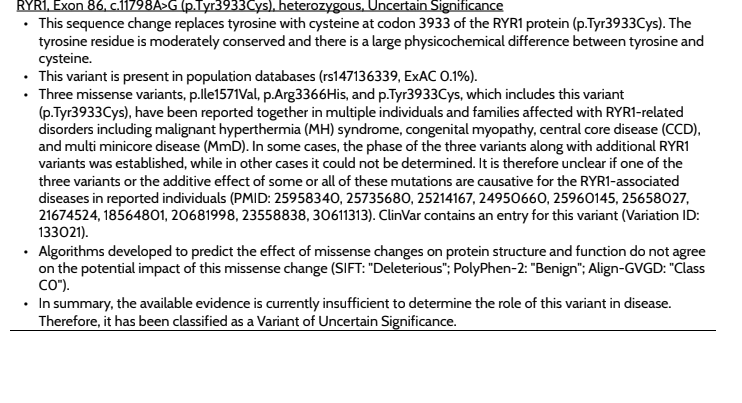
RYR1, Exon 86, c.11798A>G (p.Tyr3933Cys), heterozygous, Variant of Uncertain Significance
Breaking Down the Name
“Exon 86” — Very late in the gene (86 of 106 exons)
- Located within or near Hotspot 3 (C-terminal, aa 4,136–4,973 approximately — though the exact hotspot boundaries vary by source, this exon encodes residues approaching that region)
- Getting close to the transmembrane/pore region of the protein
- This region is highly conserved across species — a sign that changes here are more likely to be damaging
“c.11798A>G” — DNA-level change
- Position 11,798 in the coding sequence
- “A>G” = Adenine replaced by Guanine
- Single nucleotide substitution — reading frame preserved
- A missense substitution at the DNA level
“p.Tyr3933Cys” — Protein-level consequence
- “Tyr” = Tyrosine — the normal amino acid at position 3,933
- “3933” = amino acid position 3,933 out of 5,037 — approximately 78% through the protein
- “Cys” = Cysteine — the amino acid introduced by this mutation
- This is a missense mutation — single amino acid substitution
The Tyrosine-to-Cysteine Change — Why This Is More Concerning Than #2
Tyrosine (Tyr, Y):
- Large aromatic (ring-containing) amino acid
- Has a hydroxyl (-OH) group on its aromatic ring
- Can form hydrogen bonds through the hydroxyl group
- Participates in protein-protein interactions through both hydrophobic stacking (aromatic ring) and hydrogen bonding (hydroxyl)
- Often found at functionally important sites — enzyme active sites, protein interaction surfaces, signaling phosphorylation sites (tyrosine is a major phosphorylation target)
Cysteine (Cys, C):
- Small amino acid with a sulfhydryl (-SH) group
- Completely different chemical character from tyrosine — different size, different charge, different reactivity
- The sulfhydryl group of cysteine can form disulfide bonds with other cysteines — structurally critical but abnormal disulfide bonds could severely disrupt protein folding
- Cysteines introduced at non-native positions can cause abnormal protein aggregation or misfolding
- The Invitae report specifically notes “there is a large physicochemical difference between tyrosine and cysteine” — this is accurate and significant
Why this substitution is more concerning than p.Arg3366His:
- Larger physicochemical difference — Tyr→Cys is a more dramatic chemical change than Arg→His
- Cysteine’s unique reactivity — an ectopic (incorrectly placed) cysteine can form aberrant disulfide bonds that misfolded the protein
- Location in a highly conserved region — amino acid 3,933 is in a region closer to the critical transmembrane domain, where the protein sequence is under stronger evolutionary pressure to remain unchanged
- The tyrosine residue at 3,933 may be functionally important — if it’s in an interdomain contact region or a post-translational modification site, replacing it disrupts that specific function
Population Frequency
- rsID: rs147136339
- ExAC frequency: approximately 0.1%
- Same frequency level as p.Arg3366His — both exist in the general population at low but non-zero frequency
Computational Predictions (Also Contradictory)
- SIFT: “Deleterious”
- PolyPhen-2: “Benign”
- Align-GVGD: “Class CO”
- Same pattern of disagreement as mutation #2
ClinVar Entry
- ClinVar Variation ID: 133021
- Multiple entries in ClinVar — has been reported in affected individuals
PROOF HERE: What the genetic test states
Mutation #4 (Paternal)
Full Designation:
RYR1, Exon 33, c.4711A>G (p.Ile1571Val), heterozygous, Variant of Uncertain Significance
Breaking Down the Name
“Exon 33” — In the first half of the gene
- Located within Hotspot 1 (approximately aa 35–614) OR between Hotspot 1 and Hotspot 2
- Actually at amino acid position 1,571 — this is PAST the canonical Hotspot 1 boundary but BEFORE Hotspot 2
- However, Hotspot boundaries are somewhat loosely defined and different papers use slightly different ranges
- This region is part of the large N-terminal cytoplasmic regulatory domain
“c.4711A>G” — DNA-level change
- Position 4,711 in the coding sequence
- “A>G” = Adenine replaced by Guanine
- Single nucleotide substitution
- Missense substitution — reading frame preserved
“p.Ile1571Val” — Protein-level consequence
- “Ile” = Isoleucine — the normal amino acid at position 1,571
- “1571” = amino acid position 1,571 out of 5,037 — approximately 31% through the protein
- “Val” = Valine — the amino acid introduced by this mutation
The Isoleucine-to-Valine Change — The Most Conservative of the Three
Isoleucine (Ile, I):
- Nonpolar, hydrophobic (water-repelling) amino acid
- Has a branched side chain
- Medium-large size
- Typically buried in the hydrophobic core of proteins
- No charge, no reactive groups
Valine (Val, V):
- ALSO nonpolar, hydrophobic amino acid
- Has a branched side chain (slightly smaller than isoleucine)
- Similar chemical character to isoleucine but slightly smaller
- Also typically buried in hydrophobic protein cores
Why this is the “mildest” of the three paternal variants:
- Very small physicochemical difference — Ile and Val are both nonpolar, hydrophobic amino acids; they are chemically very similar
- No change in charge, polarity, or reactivity — unlike the Arg→His or Tyr→Cys changes
- The Invitae report notes “small physicochemical difference” for this variant — consistent with the chemistry
- Highest population frequency (0.5%) among the three paternal VUS variants — 1 in 200 people in ExAC carry this variant
Why it is NOT considered benign despite seeming mild:
- Isoleucine 1,571 is highly conserved — the Invitae report specifically notes “the isoleucine residue is highly conserved” — meaning natural evolution has strongly preserved this amino acid at this position across many species, suggesting changes here disrupt important function
- It travels with two other more impactful variants on the same allele — the cumulative effect of all three variants together on the same chromosome may be synergistic
- It has been reported as part of the trio in affected individuals — though the three-variant cluster’s individual contribution cannot be fully disentangled
- Location in a regulatory domain — even conservative amino acid changes in critical regulatory positions can alter allosteric signaling
Population Frequency
- rsID: rs146429605
- ExAC frequency: approximately 0.5% — the most common of your four RYR1 variants (excluding the novel null allele which has zero frequency)
Computational Predictions
- SIFT: “Deleterious”
- PolyPhen-2: “Benign”
- Align-GVGD: “Class CO”
- Same contradictory pattern as mutations #2 and #3
ClinVar Entry
ClinVar Variation ID: 159851
PROOF HERE: what the genetic report states
THE THREE-VARIANT HAPLOTYPE — THE CRITICAL CONCEPT
The most important thing about mutations #2, #3, and #4 is that they are all on the same chromosome — they form a haplotype (a set of variants that are inherited together as a single unit).
Why This Matters More Than Any Individual Variant
Consider the analogy of a recipe for a complex dish. One unusual ingredient substitution might be harmless. But three simultaneous unusual substitutions in the same recipe — one changing the salt, one changing the fat, and one changing the thickener — could interact to produce something entirely different from the intended dish, even if each substitution alone seemed minor.
Similarly, when three missense variants exist on the same RYR1 allele:
- Each variant individually makes a small structural change to the protein
- But these three changes are present SIMULTANEOUSLY in the same protein molecule
- Their effects may be additive (each adding a small disruption)
- Or synergistic (each change making the other changes worse)
- Or they may affect different functional aspects of the protein that together disrupt it more completely than any one would alone
Variant 4 (p.Ile1571Val) — in the N-terminal regulatory domain, potentially affecting allosteric regulation signals
Variant 2 (p.Arg3366His) — in the inter-domain communication region, potentially affecting signal transmission
- Variant 3 (p.Tyr3933Cys) — approaching the transmembrane domain, potentially affecting channel gating and calcium selectivity
Together on one allele, these three variants may produce a protein that:
- Receives regulatory signals abnormally (due to variant 4)
- Transmits those signals poorly (due to variant 2)
- Gates abnormally and may have altered calcium conductance or an aberrant disulfide bond (due to variant 3)
The Family Evidence That Makes This Trio Significant
The Invitae report cites multiple published PMIDs where exactly these three variants — p.Ile1571Val, p.Arg3366His, and p.Tyr3933Cys — have been reported TOGETHER in individuals and families with:
- Malignant hyperthermia syndrome (MHS)
- Congenital myopathy
- Central core disease (CCD)
- Multiminicore disease (MmD)
In some of those families, the phase (whether the three variants were on the same or different chromosomes) was established, and the trio was confirmed as a disease-associated haplotype. In others, phase could not be determined.
The fact that this specific combination of three variants has been seen in multiple unrelated affected families is strong evidence that the trio together is clinically significant — even though no individual variant alone meets the threshold for Pathogenic or Likely Pathogenic classification.
MY situation adds to this evidence: I have all three variants on MY paternal allele (confirmed in cis by family history), AND I have a null maternal allele, AND I have a clinical presentation consistent with recessive RYR1 myopathy. This is exactly the pattern that builds the case for reclassifying the trio from VUS to Likely Pathogenic.
MY FIFTH MUTATION — THE PLEC VUS
Full Designation:
- PLEC, Exon 32, c.6271_6282del (p.Glu2091_Gln2094del), heterozygous, Variant of Uncertain Significance
What Is PLEC
PLEC encodes the protein Plectin — a very large cytoskeletal linker protein (one of the largest in the human body, even larger than RYR1 at approximately 4,684 amino acids in its major isoform).
Plectin functions as a molecular scaffold and mechanical linker — it connects different cytoskeletal networks together:
- Connects intermediate filaments to the sarcolemma (muscle cell outer membrane)
- Connects intermediate filaments to the nuclear membrane
- Connects intermediate filaments to desmosomes and hemidesmosomes (cell junction structures)
- Helps distribute mechanical forces across the cell to prevent damage during muscle contraction
- Critical for muscle cell structural integrity during the repeated stress of contraction
Plectin is expressed in:
- Skeletal muscle (highly expressed)
- Skin (particularly the dermal-epidermal junction)
- Heart
- Neurons
- Many other tissues
PLEC-Related Diseases
Because PLEC is expressed in multiple tissues, PLEC mutations cause a diverse group of conditions depending on which tissues are most affected:
- Autosomal recessive conditions (both copies affected):
Epidermolysis Bullosa Simplex with Muscular Dystrophy (EBS-MD) — skin blistering from birth (due to skin junction failure) plus progressive muscle disease; MedGen UID 347335 - Epidermolysis Bullosa Simplex with Pyloric Atresia (EBS-PA) — skin blistering plus narrowing of the stomach outlet; MedGen UID 436922
- Epidermolysis Bullosa Simplex with Myasthenic Syndrome (EBS-MS) — skin blistering plus neuromuscular junction dysfunction (muscle weakness); PMID 21263134
- Limb-Girdle Muscular Dystrophy Type 2Q (LGMD2Q) — muscle disease affecting primarily the shoulder and hip girdle muscles, WITHOUT skin involvement; MedGen UID 462339
Autosomal dominant condition (one copy sufficient):
- Epidermolysis Bullosa Simplex, Ogna type (EBS-Ogna) — a milder skin fragility disorder; MedGen UID 98488
Breaking Down MY PLEC Mutation
“Exon 32” — One of PLEC’s many exons (PLEC has alternative splicing producing multiple isoforms, so exon numbering can vary by transcript used)
“c.6271_6282del” — DNA-level change
- “c.6271_6282” = a range of coding sequence positions from 6,271 to 6,282
- “del” = deletion
- 6,282 − 6,271 + 1 = 12 nucleotides deleted
- This is a 12-nucleotide in-frame deletion — critically different from MYmaternal RYR1 frameshift
“p.Glu2091_Gln2094del” — Protein-level consequence
- “Glu2091” = Glutamic acid at position 2,091 (first deleted amino acid)
- “Gln2094” = Glutamine at position 2,094 (last deleted amino acid)
- “del” = deletion of this stretch
- FOUR AMINO ACIDS (Glu-2091 through Gln-2094) are deleted from the plectin protein
- The reading frame IS preserved (12 nucleotides = 4 complete codons; deleting complete codons maintains the reading frame)
The In-Frame Deletion Mechanism
Because 12 nucleotides = exactly 4 complete codons, this deletion removes exactly 4 amino acids from the plectin protein while leaving the rest of the sequence intact. This is fundamentally different from MY maternal RYR1 frameshift:
- RYR1 frameshift: 1 nucleotide deleted → all subsequent codons scrambled → nonsense-mediated decay → no protein
- PLEC in-frame deletion: 12 nucleotides deleted → 4 amino acids missing → rest of protein sequence intact → protein IS made but is missing 4 amino acids
A protein missing 4 amino acids can potentially:
- Fold nearly normally (if those 4 amino acids are in a non-critical region)
- Have subtly altered function (if those amino acids are in a moderately important region)
- Have significantly altered function (if those amino acids are in a critical domain)
- Fail to fold properly (if those amino acids are essential for structural stability)
Why This PLEC Variant Is Classified VUS
Several specific reasons from the Invitae report:
“The frequency data for this variant in the population databases is considered unreliable, as metrics indicate poor data quality at this position in the ExAC database”
This means the ExAC/gnomAD data at this genomic position has technical artifacts that make the frequency numbers untrustworthy — can’t use population frequency as evidence
No literature reports:
- “This variant has not been reported in the literature in individuals with PLEC-related conditions”
- Unlike the RYR1 trio which has appeared in affected families, this PLEC variant has no published clinical associations
No experimental data:
- “Experimental studies and prediction algorithms are not available or were not evaluated for this variant”
- No functional studies have been done on this specific variant
- The functional significance of the affected amino acids (Glu2091-Gln2094) is currently unknown
Clinical Significance for ME
At this time, this PLEC variant is considered a finding of uncertain significance that:
- Is being monitored but NOT treated or managed specifically
- Does NOT by itself explain your clinical presentation
- Would require both copies of PLEC to be mutated for the recessive muscle conditions (LGMD2Q, EBS-MD, etc.) — I have only ONE copy affected
- May be a completely benign variant that happens to have been found alongside MY RYR1 variants
- Would require future functional studies or additional cases to be reclassified
- Is relevant to MY mother/father/half-sibling if any of them were tested, as it might help understand whether this is a family variant
PROOF: what the report states
THE COMPOUND HETEROZYGOUS PICTURE — ALL VARIANTS TOGETHER
- CHROMOSOME 19 — MATERNAL COPY:
- [Normal RYR1]—-[EXON 90: c.12567del]—-[Normal rest of gene]
- ↓
- FRAMESHIFT → PREMATURE STOP → NMD → ZERO PROTEIN
- = Complete loss of function on this allele
- CHROMOSOME 19 — PATERNAL COPY:
- [EXON 33: c.4711A>G]—-[EXON 67: c.10097G>A]—-[EXON 86: c.11798A>G]
- (p.Ile1571Val) (p.Arg3366His) (p.Tyr3933Cys)
- ↓
- ALTERED RYR1 PROTEIN — all three changes present simultaneously
- = Protein is made but with potentially significant functional alterations
- = The only source of any RYR1 protein in MY muscle cells
- CHROMOSOME (unknown) — ONE COPY:
- PLEC c.6271_6282del (p.Glu2091_Gln2094del)
- = In-frame deletion of 4 amino acids from plectin protein
- = Significance unknown; recessive disease requires BOTH copies affected
-
Net result: MY skeletal muscle cells have:
- Zero functional RYR1 from the maternal allele
- Only the three-VUS-harboring protein from the paternal allele
- This single source of RYR1 protein must supply ALL the calcium release channel function for EVERY muscle cell in MY body
- If the paternal allele’s protein has reduced function (plausible given the three simultaneous missense changes), she has significantly sub-normal total RYR1 channel function
- Plus MH susceptibility from both the null allele and the paternal variants (the trio has appeared in MH-affected families)
I WANTED TO SHARE MY RESULTS AND PROOF OF SO THAT IF ANYONE WHO HAS THE SAME EXACT MUTATIONS AS ME PLEASE REACT OUT AS IN THE DATABASE I APPEAR TO BE THE ONLY ONE WITH THE MATERNAL MUTATION WHICH CAN INDICATE MY SYMPTOMS COULD BE DIFFERENT THEN OTHERS AS THIS IS A NOT KNOWN VARIANT
Please feel free to comment! Part TWO will come out soon

