

Welcome Back!
Here i will explain all of the risk factors of RYR1 and PLEC mutations including drug side affects and Malignant Hyperthermia!
The List
Major
- Malignant Hyperthermia (MH) & Anesthesia Risk
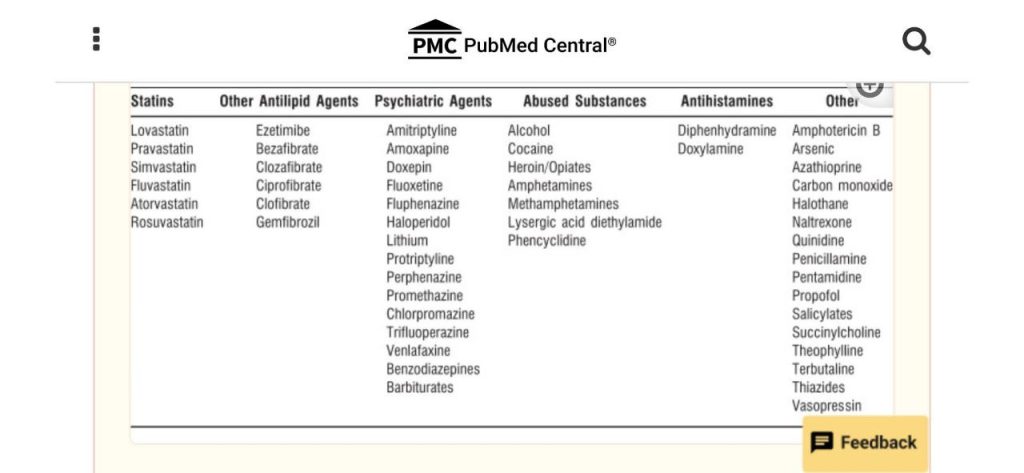
- Medication Side Effects & Sensitivities
- Statins
- psychiatric agents
- abused substance
- antihistamines
- Physical & Environmental Risks
Malignant Hyperthermia
Explaining why MH happens!
Malignant Hyperthermia (MH) is essentially a “perfect storm” where a genetic mutation meets specific medical triggers. It’s not a disease you “catch,” but rather a latent trait in your DNA that stays hidden until you’re exposed to specific anesthesia.
The Genetic “Why”
- MH is caused by a mutation in the genes responsible for how your muscle cells handle calcium. The most common culprit is the RYR1 gene
- In a healthy body, muscle contraction and relaxation are governed by the precise release and reabsorption of calcium ions. If you have the MH mutation, the “gatekeeper” protein that manages this calcium is structurally flawed.
The Protein Trigger: The RyR1 Receptor
The protein involved is the Ryanodine Receptor 1 (RyR1). Think of this protein as a high-pressure floodgate located on a storage tank (the sarcoplasmic reticulum) inside your muscle cells.
- The Normal State: When you want to move, the gate opens briefly, calcium floods the muscle cell to cause a contraction, and then the gate shuts so the calcium can be pumped back into storage.
- The Trigger: When a person with this mutation is exposed to volatile anesthetic gases (like Sevoflurane or Desflurane) or the muscle relaxant Succinylcholine, these drugs bind to the mutated RyR1 protein.
- The Failure: Instead of a controlled opening, the trigger causes the mutated RyR1 protein to get stuck in the “open” position.
The Chain Reaction
Once that protein gate is stuck open, the following happens:
- Calcium Overload: Calcium pours into the muscle cell uncontrollably.|
- Constant Contraction: The muscles lock up in a massive, sustained contraction (rigidity).
- Metabolic Overdrive: Your body burns through energy (ATP) at an impossible rate trying to pump the calcium back out and maintain the contraction.
- Heat and Acid: This hyper-metabolic state generates massive amounts of heat (leading to the “Hyperthermia”) and lactic acid, eventually causing muscle cells to burst and leak potassium into the bloodstream, which can stop the heart.

The Ryanodine Receptor 1 (RyR1) is actually one of the largest proteins in the human body. Because it is so massive and complex, it is often described as looking like a mushroom or a four-leaf clover.
Key Features of the RyR1 Protein:
- The “Mushroom” Shape: The large “cap” of the mushroom sits inside the fluid of the muscle cell (the cytoplasm). This is where the anesthetic gases bind to the protein.
- The “Stem”: The stem part of the protein is embedded in the membrane of the sarcoplasmic reticulum (the storage tank for calcium). This part contains the actual pore or “gate.”
- Four Subunits: The protein is made of four identical parts that join together. In the center of these four parts is the hole that allows calcium to flow through.
How it fails in Malignant Hyperthermia:
In a person with the MH mutation, the protein structure is slightly unstable. When the trigger (like anesthesia) hits the “cap” of the protein, the physical shape shifts. Instead of clicking shut after a second, the “stem” (the pore) stays wide open. This acts like a broken dam, allowing a flood of calcium to pour into the muscle, which causes the dangerous symptoms of MH.
Explaining the list of drugs that causes triggers and why
Malignant Hyperthermia (MH) is only triggered by two specific classes of drugs. If you or a family member are “MH Susceptible,” these are the drugs that must be strictly avoided.
Inhaled Volatile Anesthetics (Gas)
These are the “potent” gases used to keep a patient unconscious during surgery. They are all halogenated (contain elements like fluorine or chlorine), which is part of why they react with the RyR1 protein.
- Sevoflurane (the most common gas used today)
- Desflurane
- Isoflurane
- Halothane (mostly used outside the US now)
- Enflurane (older, rarely used)
- Methoxyflurane (older)
- Ether (historical)
Depolarizing Muscle Relaxants
There is really only one primary drug in this category still in common use that triggers MH. It is used to temporarily paralyze muscles for intubation (inserting a breathing tube).
- Succinylcholine (also called Suxamethonium or “Succs”)
Always make sure the hospital have Dantrolene
What is SAFE? (The Non-Triggers)
It is just as important to know what doesn’t cause a reaction, so you know what can be used instead. The following drugs do not interact with the “glitchy” calcium protein:
- IV Anesthetics: Propofol, Ketamine, Etomidate, and Barbiturates (like Thiopental).
- Safe Gases: Nitrous Oxide (Laughing Gas) and Xenon.
- Non-depolarizing Muscle Relaxants: Rocuronium, Vecuronium, Cisatracurium, and others.
- Local/Regional Numbing: Lidocaine, Bupivacaine, etc. (Epidurals and Spinals are safe).
- Pain & Anxiety Meds: All opioids (Fentanyl, Morphine) and Benzodiazepines (Versed/Midazolam).
Important Note: If you are asking because you have a surgery coming up, you should tell your anesthesiologist: “I have a concern about Malignant Hyperthermia history.” They will perform a “Trigger-Free Anesthetic” using the safe list above and will prep the anesthesia machine to ensure no trace amounts of gas are present.
Beyond the standard anesthetic gases and the muscle relaxant succinylcholine, there is a very short list of other substances and situations that can trigger a Malignant Hyperthermia (MH) event or a very similar reaction.
Researchers sometimes refer to these as “Awake MH” triggers because they can happen outside of a hospital setting.
Recreational Drugs (Specifically MDMA)
MDMA (Ecstasy) is the most significant non-medical drug trigger.
- The Reaction: People with the RYR1 mutation are much more likely to suffer fatal “overheating” when taking MDMA.
- The Reason: MDMA triggers the same calcium leak in the muscles that anesthesia does. Many cases of “Ecstasy-related deaths” are actually undiagnosed Malignant Hyperthermia.
Statins (Cholesterol Medication)
Statins (like Simvastatin or Atorvastatin) are not “primary” triggers like anesthesia, but they have a complex relationship with MH.
- Unmasking: Some studies suggest that statins can “unmask” a latent muscle problem. If you have the MH mutation, statins might cause muscle breakdown (rhabdomyolysis) or lower your threshold for a reaction if you are later exposed to anesthesia.
High-Intensity Exercise & Heat
This is often called Exertional Heat Stroke (EHS), and it is closely linked to the same genetic “glitch” as MH.
- The Trigger: Extremely vigorous physical activity, especially in hot and humid environments.
- The Result: The “gatekeeper” protein (RyR1) fails due to the stress and heat of the workout, leading to muscle rigidity and a spike in body temperature that looks exactly like an MH crisis in surgery.
Caffeine (In extreme amounts)
In the laboratory, doctors use caffeine to force a muscle biopsy to contract to see if you have MH.
- In Daily Life: You don’t need to worry about a cup of coffee. However, “mega-doses” (like those found in some high-potency pre-workout supplements or caffeine pills) could theoretically aggravate the RyR1 protein in someone who is highly susceptible.
Important: The “Look-Alikes”
There are other drugs that cause a similar “overheating” crisis, but they are not Malignant Hyperthermia, even though they look the same. They affect the brain rather than the muscle protein directly:
- Antipsychotics (Haloperidol, etc.): Can cause Neuroleptic Malignant Syndrome (NMS). It looks like MH, but the “glitch” is in the brain’s dopamine system, not the muscle’s calcium gates.
- Antidepressants (SSRIs): Can cause Serotonin Syndrome, which also involves high fever and muscle rigidity but is caused by too much serotonin.
Now explaining the symptoms of a MH flare
In the medical world, an MH “flare” is called a Malignant Hyperthermia Crisis. Because it is a hyper-metabolic reaction, the body essentially goes into “overdrive.”
It is important to know that high fever is actually a late sign. Doctors look for other clues first because once the fever spikes, the body is already in a dangerous state.
Early Warning Signs (The First Clues)
These usually happen within minutes of being exposed to the trigger drugs:
- Masseter Muscle Rigidity (MMR): This is one of the most famous signs. The jaw muscles lock up so tightly that the doctor cannot open the patient’s mouth to insert a breathing tube.
- Rapid Heart Rate (Tachycardia): The heart starts racing as it tries to keep up with the body’s sudden demand for oxygen.
- Spike in Carbon Dioxide ($CO_2$): This is often the very first sign a doctor sees on their monitors. The body is burning energy so fast that it produces a massive amount of waste gas (CO_2).
- Rapid Breathing: If the patient isn’t paralyzed, they will start breathing very fast and shallow.
The “Active” Crisis Symptoms
As the reaction continues and the muscle cells begin to break down, you see:
- Generalized Muscle Rigidity: It’s not just the jaw anymore; the entire body may become stiff or “board-like.”
- Mottled or Flushed Skin: The skin may look patchy, purple, or bright red as blood flow shifts and the body tries to dump heat.
- Unstable Blood Pressure: It may swing wildly from high to low.
Late-Stage Symptoms (The Danger Zone)
If the reaction isn’t stopped quickly with the antidote (Dantrolene), these severe symptoms occur:
- Extreme High Temperature: The temperature can rise at a rate of $1^{\circ}C$ to $2^{\circ}C$ every five minutes, sometimes reaching over 110°F (43.3°C).
- Cola-Colored Urine: This is a sign of Rhabdomyolysis. The muscle cells are bursting and releasing a protein called myoglobin into the blood, which stains the urine dark brown or tea-colored. This can lead to kidney failure.
- Cardiac Arrhythmia: The bursting muscle cells also leak Potassium into the blood. Too much potassium causes the heart to beat out of rhythm or stop entirely.
What happens in “Awake MH”?
If this happens outside of surgery (due to extreme heat or exercise), the person will feel:
- Extreme, painful muscle cramping (worse than a normal cramp).
- An overwhelming sense of heat or “burning up.
- Dark-colored urine later that day or the next morning.
Medication Side Effects & Sensitivities
Statins
The reason statins create a “danger zone” for people with RYR1 or PLEC mutations comes down to cell stability. If your muscle cells already have a structural or chemical “glitch,” adding a statin is like putting a heavy load on a cracked foundation.
Statins are designed to lower cholesterol, but they also affect the mitochondria (the power plants) and the membranes (the walls) of your muscle cells.
RYR1: The Calcium “Leaking” Problem
As we discussed, the RYR1 protein is the gatekeeper for calcium. Even if you haven’t had an MH crisis, a mutated RYR1 gate might be “leaky,” allowing tiny amounts of calcium to drip out when they shouldn’t.
- The Statin Interaction: Statins decrease the production of CoQ10, which mitochondria need to produce energy. They can also directly interfere with how calcium is pumped back into storage.
- The “Double Hit”: If the RyR1 gate is already leaky, and the statin makes it harder for the cell to pump that calcium back out (due to low energy), the muscle cell becomes overwhelmed.
- The Result: This leads to Statin-Induced Myopathy (muscle pain) or even Rhabdomyolysis (muscle breakdown). Essentially, the statin “unmasks” the RYR1 mutation, turning a hidden genetic trait into an active medical problem.
PLEC: The Structural “Glue” Problem
The PLEC gene codes for a protein called Plectin. Plectin is basically the “universal glue” or “rebar” of the muscle cell. It anchors the internal machinery of the cell to the outer skin (the sarcolemma).
- The Mutation: If you have a PLEC mutation, your muscle fibers are physically fragile. They don’t handle mechanical stress or chemical changes very well.
- The Statin Interaction: Statins are known to alter the lipid (fat) composition of cell membranes. This can make the “skin” of the muscle cell more fluid or less stable.
- The “Double Hit”: When you take a statin, the cell membrane becomes slightly more vulnerable. If the “rebar” (Plectin) holding that membrane in place is already weak, the cell is much more likely to rupture or “pop” during normal activity.
- The Result: This often manifests as severe muscle weakness or a type of muscular dystrophy that is significantly worsened by cholesterol medication.
Statin Drug List
(High Risk)
These statins enter muscle cells through passive diffusion and have been shown in recent studies to bind directly to the RyR1 receptor, causing the dangerous calcium leak we discussed.
- Atorvastatin (Lipitor): Recent high-level research (2025/2026) has identified this as a direct binder to RyR1, destabilizing the gate and promoting calcium leaks.
- Simvastatin (Zocor): Widely considered the most “muscle-toxic” statin for those with genetic vulnerabilities.
- Lovastatin (Mevacor, Altoprev): Highly lipophilic and similar in structure to simvastatin.
- Fluvastatin (Lescol): Also lipophilic with a moderate risk of muscle interaction.
- Pitavastatin (Livalo): While potent, it is lipophilic and carries a higher risk for muscle-sensitive patients.
(Low Risk)
If a statin is absolutely necessary, doctors typically switch to hydrophilic (water-soluble) statins. These do not “leak” into muscle cells easily; they stay in the bloodstream and are mostly taken up by the liver.
- Pravastatin (Pravachol): Generally considered the safest for people with RYR1/muscle issues. It has almost zero affinity for the RyR1 receptor.
- Rosuvastatin (Crestor): While very powerful, it is hydrophilic. It is much less likely to cause muscle issues than Lipitor or Zocor, but should still be used at the lowest effective dose.
Non-Statin Alternatives (Muscle-Safe)
For many people with RYR1 or PLEC mutations, doctors may move away from the statin class entirely to avoid any risk of “unmasking” a muscle crisis. These drugs work differently and do not affect the RyR1 calcium gate:
- Ezetimibe (Zetia): Works in the gut to stop cholesterol absorption. It has no known interaction with muscle proteins.
- PCSK9 Inhibitors (Repatha, Praluent): These are injectable medications that are highly effective and are generally considered the “gold standard” for patients who cannot tolerate statins due to muscle pain.
- Bempedoic Acid (Nexletol): A newer drug that is only activated in the liver, meaning it technically cannot affect muscle tissue.
Crucial Warning: If you have an RYR1 or PLEC mutation and are prescribed a statin, you should ask your doctor for a baseline Creatine Kinase (CK) blood test. This allows them to monitor if the drug is causing “silent” muscle breakdown before it becomes a full-blown crisis.
Psychiatric Agents
To give you the full picture, we have to look at how these drugs hit the muscle from two different directions: the chemical “gate” (RYR1) and the physical “frame” (PLEC).
Whether it’s a true Malignant Hyperthermia (MH) event or a “Non-MH” reaction, the result is often the same: muscle breakdown and dangerous metabolic shifts.
MH-Related Reasons (The Calcium “Flood”)
In these cases, the drug acts as a key that accidentally unlocks the RYR1 calcium gate
- Destabilization of the Receptor: Some psychiatric drugs, especially “Typical” antipsychotics (like Haloperidol), can interfere with the stability of the RyR1 protein. If your gate is already “leaky” due to a mutation, these drugs can push it into an “open” state.
- The “Second Hit” Theory: You might be able to handle a RYR1 mutation or a specific drug alone, but the combination of the two creates a “perfect storm.” The drug causes the brain to send constant signals for the muscles to contract; the mutated RyR1 gate can’t handle that constant signaling and gets stuck open, triggering a full MH-like crisis (Neuroleptic Malignant Syndrome).
Non-MH Reasons (The Structural and Metabolic “Burnout”)
These issues happen even if the calcium gate stays closed. They focus on the physical strength of the cell (PLEC) and the brain’s control over the muscles.
Physical “Tearing” (The PLEC Problem)
The PLEC gene makes Plectin, the “rebar” that holds muscle fibers together.
- Extrapyramidal Side Effects (EPS): Many psych drugs cause involuntary movements (tremors, twitching, or “pill-rolling”).
- Mechanical Stress: In a normal person, a tremor is just annoying. In someone with a PLEC mutation, the muscle “frame” is fragile. Constant twitching or rigid “clenching” from a drug literally tears the muscle cells apart because the plectin isn’t there to support the internal structure.
The Mitochondrial “Power Failure”
Many psychiatric agents and antilipid agents (statins) are mitochondrial toxins.
- Energy Depletion: These drugs can decrease the production of ATP (cellular fuel).
- The Result: Muscle cells need massive amounts of ATP to keep their “pumps” running to stay alive. If the drug drains the battery, and the cell is already genetically weak (RYR1/PLEC), the cell simply “pops” and dies, leading to high CK levels and pain.
The Brain-Body “Short Circuit”
- Dopamine Blockade: Drugs that block dopamine (antipsychotics) cause the body to become rigid like a “lead pipe.”
- Heat Generation: This intense rigidity generates massive amounts of heat through friction and metabolism. This heat can physically warp proteins—including the mutated RyR1—triggering a secondary calcium leak even if the drug didn’t hit the protein directly.
If you have these mutations, these “Non-Anesthetic” drugs are the ones to watch:
- Antipsychotics: Especially “Typical” ones (Haldol, Thorazine).
- Lithium: Can worsen muscle tremors and metabolic stress.
- High-Dose SSRIs: Can cause “Serotonin Syndrome,” which mimics MH symptoms.
- Statins: Drains the energy needed to fix minor calcium leaks.
Drug List
High-Risk: “Typical” Antipsychotics
- Haloperidol (Haldol): The #1 most common trigger for drug-induced muscle crisis in psychiatric patients.
- Fluphenazine (Prolixin)
- Chlorpromazine (Thorazine)
- Thioridazine (Mellaril)
- Trifluoperazine (Stelazine)
- Perphenazine (Trilafon)
Moderate-Risk: “Atypical” Antipsychotics
- Risperidone (Risperdal): Frequently linked to NMS cases.
- Olanzapine (Zyprexa)
- Quetiapine (Seroquel)
- Aripiprazole (Abilify)
- Clozapine (Clozaril)
- Ziprasidone (Geodon)
Other Dangerous Add-Ons
- Lithium: Often used for Bipolar Disorder. It can increase the risk of NMS when taken with the drugs listed above and can cause muscle tremors that stress PLEC mutations.
Antiemetics (Nausea Meds): Believe it or not, some nausea meds are “hidden” neuroleptics.
- Metoclopramide (Reglan)
- Prochlorperazine (Compazine)
- Promethazine (Phenergan)
Dopamine Withdrawal:
- Abruptly stopping Parkinson’s meds like Levodopa or Amantadine can trigger a “withdrawal NMS” that looks exactly like an MH crisis.
Abused Substances
Abused substances—specifically stimulants and “club drugs”—are arguably the most dangerous non-surgical triggers for people with
Unlike medical drugs, these substances often hit the body with massive, uncontrolled surges of chemicals that can trigger a crisis even without the presence of anesthesia.
The MH-Related Path: MDMA and “Chemical Overdrive”
MDMA (Ecstasy/Molly) is the primary “abused” trigger. It interacts with the RYR1 protein in a way that mimics an anesthesia crisis.
- The Direct Interaction: MDMA causes a massive release of serotonin and dopamine. This doesn’t just happen in the brain; it affects the signaling at the neuromuscular junction.
- Destabilizing the Gate: High levels of serotonin and increased body temperature physically “warp” the already unstable RyR1 protein. The mutated gate “pops” open, leading to a massive calcium leak.
- The Result: A full-blown “Awake MH” crisis. The user develops “lead-pipe” rigidity, their body temperature can spike to 108°F+, and their muscles begin to liquefy (rhabdomyolysis).
The Non-MH Related Path: Cocaine, Meth, and “Mechanical Failure”
Substances like Cocaine and Methamphetamine cause issues regardless of whether a “classic” MH event occurs, especially for those with PLEC mutations.
Extreme Mechanical Stress (The PLEC Problem)
Stimulants cause intense, repetitive movements: teeth grinding (bruxism), tremors, and severe muscle clenching
- The Structural Collapse: If your PLEC gene is mutated, your muscle cells lack the “rebar” needed to handle this stress. The constant, high-tension clenching literally shatters the muscle fiber membranes.
- The Result: Severe muscle pain and a massive spike in Creatine Kinase (CK) levels as the cell contents spill into the blood.
Mitochondrial Poisoning & Vasoconstriction
- Lack of Oxygen: Cocaine causes blood vessels to narrow (vasoconstriction). This starves the muscles of oxygen.
- Energy Depletion: Without oxygen, the cell can’t make ATP. As we discussed, if the cell runs out of ATP, it can’t pump calcium back into storage. Even a “minor” RYR1 leak becomes fatal because the cell doesn’t have the energy to “mop up” the extra calcium.
Drug List
The “Awake MH” Triggers (RYR1 Risk)
- MDMA (Ecstasy, Molly): The most dangerous. It causes massive serotonin release and hyperthermia, which can directly trigger an MH-like crisis.
- “Bath Salts” (Synthetic Cathinones): Drugs like Mephedrone or MDPV cause extreme agitation and “excited delirium,” leading to the same runaway calcium leak as seen in MH.
- High-Dose Caffeine: While coffee is fine, pure caffeine powder or highly concentrated “energy shots” used as stimulants can lower the threshold for a RyR1 leak.
The Muscle-Shattering Stimulants (PLEC & RYR1 Risk)
- Cocaine: Causes severe vasoconstriction (shrinking of blood vessels). This starves muscle cells of the oxygen they need to keep their calcium pumps running.
- Methamphetamine (Meth, Speed): Causes prolonged, intense muscle clenching and high body temperature. If your Plectin (PLEC) “rebar” is weak, the muscle fibers physically tear under this stress.
- Synthetic Cannabinoids (K2, Spice): These can cause seizures and severe muscle tremors, which are physically devastating to fragile muscle cell structures.
The “Look-Alike” Triggers
- PCP (Phencyclidine): Causes “muscle rigidity” and extreme physical exertion. This leads to massive spikes in Creatine Kinase (CK), which can be fatal for those with PLEC mutations.
- Alcohol (in Binge Quantities): Ethanol is a direct muscle toxin. In high doses, it can interfere with the cell membrane and mitochondria, making a “leaky” RYR1 gate even harder to manage.
Antihistamines
Antihistamines are generally considered “safe” for most people, but for those with RYR1 or PLEC mutations, specific types—especially older, “first-generation” ones—can cause significant problems.
The risk isn’t that they trigger a classic MH crisis like anesthesia does, but rather that they interfere with temperature regulation and muscle stability.
MH-Related: The “Thermostat” Problem
For someone with an RYR1 mutation, the body’s ability to handle heat is already fragile.
- The Anticholinergic Effect: Many antihistamines (like Benadryl) have “anticholinergic” properties. This means they shut down the body’s ability to sweat.
- The Heat Trap: If you cannot sweat, you cannot dump heat. For a person with RYR1 mutations, whose muscles may already be generating a slight “background” heat due to minor calcium leaks, this creates a heat trap.
- The Trigger: As your core temperature rises because you can’t sweat, the heat itself can physically destabilize the mutated RyR1 protein, causing it to “pop” open. This can lead to an “Awake MH” event or exertional heatstroke.
Non-MH Related: Muscle “Jitters” and Structural Stress
This is where the PLEC gene and general muscle health come into play.
- Restless Legs and Twitching: First-generation antihistamines are notorious for causing “Extrapyramidal Symptoms” (EPS) or severe restless leg syndrome in sensitive individuals.
- Mechanical Wear and Tear: In a person with a PLEC mutation, the muscle fibers are structurally weak. The involuntary twitching, “internal jitters,” or spasms caused by the antihistamine put constant mechanical stress on the muscle cell’s “skin” (the membrane).
- Cell Rupture: Without enough Plectin to act as “rebar,” this constant twitching can cause micro-tears in the muscle, leading to elevated Creatine Kinase (CK) levels and muscle pain (myalgia).
Why Second-Generation is Safer
Newer antihistamines like Loratadine (Claritin), Cetirizine (Zyrtec), and Fexofenadine (Allegra) are “peripheral.” They do not cross the blood-brain barrier as easily and have much lower anticholinergic effects. They generally do not interfere with sweating or cause the same level of muscle twitching, making them the preferred choice for people with RYR1 or PLEC mutations.
Drug List
The “Red Flag” List (Avoid or Use with Caution)
- Diphenhydramine (Benadryl): The most common offender. It is a potent anticholinergic that stops sweating and can cause significant muscle twitching.
- Promethazine (Phenergan): This is technically an antihistamine but is chemically related to antipsychotics. It carries a higher risk of triggering Neuroleptic Malignant Syndrome (NMS) or severe muscle rigidity.
- Hydroxyzine (Vistaril, Atarax): Often prescribed for anxiety or severe itching; it has strong effects on the central nervous system and can lead to tremors.
- Dimenhydrinate (Dramamine): Used for motion sickness; it is a derivative of diphenhydramine and has the same heat-trapping risks.
- Chlorpheniramine (Chlor-Trimeton): Frequently found in “All-in-One” cold and flu liquids (like NyQuil or Coricidin).
- Cyproheptadine (Periactin): Sometimes used to increase appetite or treat serotonin syndrome, but its complex interaction with receptors can be unpredictable for RYR1-susceptible individuals.
Safe list
- Loratadine / Claritin
- Cetirizine / Zyrtec
- Fexofenadine / Allegra
- Levocetirizine / Xyzal
- Desloratadine / Clarinex
Physical & Environmental Risks
The WHY?
When you have RYR1 or PLEC mutations, your muscles are essentially “operating on the edge.” Physical and environmental stressors act as the final push that can cause the muscle’s chemistry (RYR1) or structure (PLEC) to fail.
Here is why certain environments and activities trigger these issues.
Heat and Humidity (The “Awake MH” Trigger)
This is the most significant environmental risk for those with RYR1 mutations. It is often referred to as Exertional Heatstroke (EHS).
- The RYR1 Failure: The RyR1 calcium gate is heat-sensitive. In a healthy person, the gate stays shut even when the body gets hot. In someone with an MH mutation, high external heat (or the inability to dump heat in high humidity) can cause the protein to physically change shape and “pop” open.
- The Result: Calcium leaks into the muscle, causing more contraction, which generates more heat. This creates a lethal feedback loop where the body temperature can skyrocket to over 106°F (41°C) without any anesthesia present.
High-Intensity Exercise (The Mechanical Stress)
This affects both genes, but it is particularly brutal for those with PLEC mutations.
- PLEC (Structural Failure): Plectin is the “rebar” that anchors your muscle fibers. During “eccentric” exercise (like running downhill or heavy lifting), your muscles are stretched while they are trying to contract. Without functional Plectin, the muscle cell membrane literally rips open under the mechanical tension.
- RYR1 (Metabolic Failure): Intense exercise demands that calcium be pumped back into storage very quickly. If the RYR1 gate is leaky, the “pump” (SERCA) has to work ten times harder. Eventually, the cell runs out of energy (ATP), the pump stops, and the muscle stays in a state of permanent, painful contraction (rigidity).
High-Dose Caffeine and Stimulants (The Chemical Primer)
Environmental exposure to high levels of stimulants—like “pre-workout” powders or extreme amounts of caffeine—acts as a “chemical primer.”
- Lowering the Threshold: Caffeine is a known agonist of the RyR1 receptor (doctors even use it in “Caffeine-Halothane Contracture Tests” to diagnose MH). High doses of caffeine make the RyR1 gate much “hairier”—meaning it takes a much smaller stressor (like a warm day or a jog) to trigger a full calcium leak.
Viral Illnesses and High Fevers
Even a standard “flu” can be a physical risk for someone with these mutations.
- The Fever Trigger: A high fever from an infection is an environmental stressor from the inside. If a child or adult with an RYR1 mutation reaches a fever of 103°F or 104°F, it can sometimes “unmask” the MH trait, leading to muscle rigidity and dark urine (rhabdomyolysis) that is much more severe than a normal flu symptom.
If you have these mutations, doctors usually recommend a “Low-Stress” lifestyle
- Pre-Cooling: If you must exercise in heat, use cooling vests or cold water.
- Hydration: Never let your electrolytes get out of balance, as this stresses the calcium pumps.
- Moderate Exercise: Focus on low-impact or steady-state cardio rather than “explosive” or “maximum effort” movements that might tear Plectin-deficient fibers.
List of things to avoid
These are the “Non-MH” risks that can still lead to Rhabdomyolysis (muscle melting) if you aren’t care
- Extreme Heat & Humidity: Especially when you cannot escape to a cool environment.
- High-Intensity Interval Training (HIIT) or “Eccentric” Exercise: Heavy lifting or downhill running that puts extreme tension on the muscle’s “structural rebar” (Plectin).
- Excessive Caffeine: Concentrated caffeine powders or “pre-workout” supplements (more than 400mg-600mg at once).
- Dehydration: Lack of water makes it impossible for the muscle’s “calcium pumps” to work efficiently.
My Story with a MH Attack
When i had my Muscle Biopsy in 2018 i didn’t know i had RYR1 or PLEC gene mutations yet nor did i know i had MH, The surgery only took about an hour.
My Mother told me that the Anesthesiologists came out and told my parents that i was going to give him a hard time because he didn’t like how my stats were looking so he switched the drug he was using a couple times and even then it was still iffy,
My parents told me that it took me hours to wake up to the point my vitals were dropping and the nurse had to force me to wake up due to my heart rate being low. Again we didn’t know what this was and if it was normal etc. but if this doctor wasn’t good and wasn’t checking on me a lot something bad really could have happened.
I’ve had multiple surgeries in the past and it would always take me a long time to wake up more then usual but never had issues in the operating room so this was the first known time. but now i know what i know i haven’t had a surgery since but boy is it very scary to think what if i need one. that’s why i will always make sure the Anesthesiologists known about MH and that they have a MH risk cart on deck with unexpired Dantrolene.
Goodbye
I want to thank you for reading again and a new post will be out shortly on De novo! feel free to leave comments.
